QUESTION FROM SOCIAL MEDIA: Do you have any knowledge about Total Knee Replacements and Fitness? Out of the medical doctrine or just rehab?
ANSWER: Yes! Of course!
As a special operations medic in internship I have had the opportunity to assist in several knee replacement surgeries. It’s quite an experience! One that the picture above just doesn’t do justice to!
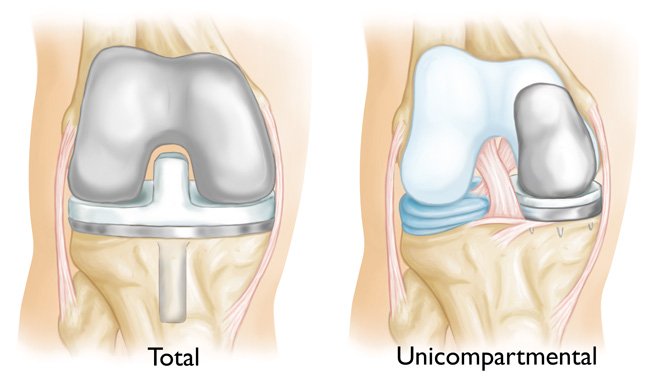
This article concerns any joint replacement procedure as the principles are identical regardless of the procedure. As I noted in my last article, any joint that allows movement is only as strong as the muscles supporting it. When a joint is surgically replaced, as seen above, we must understand that returning to a “normal” state is going to be challenging but not impossible.
First let’s address the issue surrounding the new hardware. Everyone is a little different, but generally speaking, most people with total knee replacement don’t run again. The reason is that the tibial component (the vertical spike) causes a lot of pain for obvious reasons. The problem is less pronounced in partial replacements, though there are still small spikes in the implant. The simple fact is that these protrusions move and damage tissue, which causes pain when subjected to the massive dynamic loads caused by running. In older populations we see the same sorts of pain caused by walking.
The best medicine for healthy joints is strong muscles; not just strong, but you need plenty of endurance as well. In the beginning, after surgery, you will be assigned to physical therapy. It is very important to understand that physical therapy is not there to get you fit. They will dismiss you as soon as they have restored as much normal FUNCTION as possible. For knee replacement that means the best range of motion they can manage and walking. Not walking well or fast, just walking. That’s a positive thing, but where do you go from there?
The answer is simple, you have to do your own recovery to regain full function. Your first goal being to walk without pain.
REMEMBER! PAIN USUALLY EQUALS TISSUE DESTRUCTION! If not, it’s caused by pressure on nerves. Both are bad.
If you can walk without pain, do so beginning with 20-100 meters and work up to 5-10km per day. It is likely that you will quickly hit a point where you feel the walking is not helping, improving, or perhaps is beginning to hurt. That is the time to start going to the gym to strengthen the muscles further and create the best support possible. Practically speaking, that means going to the gym and starting with light loads on machines. Following the standard rules of progression, you gradually increase the load as your muscles get stronger, ensuring you are not working through pain. Pain is bad. Pain means damage is being done.
Resistance training should begin with one day per week and increase to three days per week as your ability to recover improves. Regarding sets and reps, start with one set of 3-5 reps and work up to one set of 20-30 reps before increasing the weight. Regarding exercises for the knee, I would stick with simple leg extensions and leg curls for the first six months. Then gradually work into leg presses or squats and assisted lunges. Always err on the side of caution and safety and be sure to check in with your doctor quarterly or every six months. All in all, don’t think for a moment that things will be anywhere close to normal for 1-2 years.
Once you and your doctor feel your leg muscles have the strength and stamina to properly support the joint, it would be very beneficial to start working on movement drills such as those found in Combat Acrobatics. If able, perform these drills and walk briskly every day while performing resistance training three times per week. How strong do you want to get? As strong as possible in every direction.
I should point out that there are a few concerns as you go along. The big one is understanding the hardware you have inside you. For example, the spike (the tibial component) in the total knee replacement. The new hardware does not have the lex and give of your original anatomy. If you start forcing the knee into positions you don’t yet have the mobility for, you will transfer that force to that spike which can then cause pain or even a fracture in the tibial head. As I said, take it easy, slow, and careful.
I hope this helps point you in the right direction. Please let me know if you want anything clarified in the comments on social media.
*The views and opinions expressed on this website are solely those of the original authors and contributors. These views and opinions do not necessarily represent those of Spotter Up Magazine, the administrative staff, and/or any/all contributors to this site.